Reviewed by Sahil Chopra, MD.
Research by Savit Malhotra and Quynh Theresa Do.
Introduction
Resuming our Crash Course on Restless Legs Syndrome (RLS) series, the next topic we will address is the use of opioids for managing severe RLS symptoms. While often considered a last-resort treatment, opioids play a crucial role in targeting those with refractory RLS. Refractory RLS is defined as the failure of standard, first-line treatments (such as medications gabapentin and pregabalin) due to the lack of efficacy or intolerable side effects that preclude their continued use.[1] In these cases, alternative medication options become necessary to provide patients with relief from their disruptive symptoms. In this article, we will dive into the background of opioids, including how they work, their role in managing severe RLS, and important safety precautions associated with these medications.
Understanding Opioids as a Medication
In severe and special cases, standard first-line treatments for RLS, such as gabapentinoids, do not work effectively for the patient. This is when medications such as opioids come in. Opioids are a class of medications that mimic the natural substances found in the opium poppy plant (scientifically known as Papaver somniferum).[2] They interact with the opioid receptors in the brain and nervous system, which can control the feeling of pain, regulate breathing rate, and manage stress responses.[3] There are many types of opioids, including natural (e.g., morphine and codeine), semisynthetic (e.g., heroin, oxycodone, hydrocodone, and oxymorphone), and synthetic (e.g., fentanyl and tramadol).[3]
Opioids are mainly prescribed as pain medication for acute or chronic pain. The side effects of taking opioids include feeling sleepy, relaxed, and sometimes euphoric. Due to these relieving symptoms, opioids can become addictive, potentially developing into a condition called opioid use disorder (which will be discussed in further detail in a section below). Beyond these initial effects, there have also been reports of gastrointestinal upset, including nausea, vomiting, and constipation.[2, 3] Critically, taking opioids can also cause respiratory depression, or slowed breathing, which can lead to low oxygen levels in the body and can be dangerous and potentially fatal. In the case of an overdose, a patient can experience respiratory arrest, also known as when breathing stops while their heart is still beating. Respiratory arrest is the primary cause of death in an opioid overdose.[4] Therefore, prescribing opioids requires careful assessment, dosage, and monitoring, only to be used in cases where the clinical benefit outweighs the risks, including significant risks of physical dependence and addiction.
The Use of Opioids for RLS
Opioids have been historically used to treat RLS for decades, but have more recently been reviewed under clinical trials for RLS.[5] Currently, according to the Mayo Clinic, opioids are utilized for refractory RLS.[1] For refractory RLS, high-potency opioids may be needed. Low-dose opioid monotherapy, or only using opioid medication, in particular, has been recommended as it was found to be “highly effective in the management of refractory RLS.”[1]
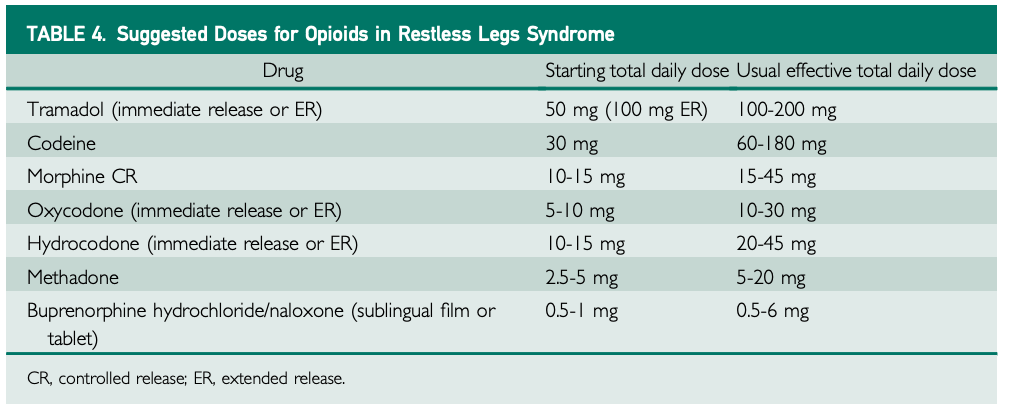
A major study on extended-release oxycodone combined with naloxone found that, after 12 weeks of treatment, patients with severe RLS who were taking this combination medication (average daily dose of about 22 mg oxycodone with 11 mg naloxone) reported improvements in their sleep quality and quantity, symptom severity, and daytime tiredness, compared to those who were taking a placebo. Naloxone is added to the oxycodone to help reduce constipation, a common side effect of opioid medications. For patients with very severe RLS symptoms lasting more than 10 hours per day, long-acting opioids such as methadone (2.5-20 mg daily) or buprenorphine (0.5-6 mg daily) may be recommended. Importantly, these doses are approximately 10% of the doses used to treat chronic pain, reflecting the lower amounts needed for RLS treatment.[6,7]
Further recommended dosages of opioids can be found in the table below.[1] It is important to note that the prescription of opioids for treating RLS depends on a variety of factors, including careful evaluation by the physician and individual patient characteristics. As emphasized, significant precautions are needed due to the risks of dependence, addiction, and the ongoing opioid crisis.
Cautionary Use of Opioids
Since the mid-to-late 1990s, the opioid epidemic has run rampant, with an estimated 79,358 deaths related to opioids in the United States in 2023.[8] Opioid use disorder (OUD, which involves the chronic use of opioids in a way that causes clinically significant distress or impairment) has been estimated to affect over 16 million people globally (2.1 million in the United States alone) and constitutes dependence or addiction to opioids.[9,10] Unfortunately, while opioids may have very effective use cases, their addictive properties prompt cautionary use.
Opioids act on a number of receptors in our brains. In particular, they bind to what are known as mu(-opioid) receptors.[11] These receptors are key to pain relief and serve as the binding site for endorphins (the body’s natural opiate).[12] When endorphins bind to these receptors, they produce analgesia (the inability to feel pain) by blocking the release of substance P, a key protein that helps to transmit pain signals, in the peripheral nervous system.[13] Opioids mimic the effects of endorphins, binding to the same receptors and leading to the same mechanism for pain blocking.[14] We will note here that, in the central nervous system, endorphins block the release of GABA, which leads to excess production of dopamine.[13]
Dopamine is known as the body’s reward and pleasure messenger and is released when we feel happy or experience a positive moment in our lives.[15] Through excess dopamine release, the body experiences the feeling of a natural high, which can cause euphoria.[16] And so while opioids can block pain signals, they also create a pathway for obtaining a high.
However, prolonged opioid use can lead to tolerance, which is when the body no longer reacts to the medication at the same level it has in the past. There are a number of theories surrounding why opioid tolerance occurs, including the receptors adapting to the opioids, changes in the way the body interacts with the drug, and opioid-induced hyperalgesia (an increased sensitivity to pain caused by an opposing system).[17] After some time, the body also becomes much more efficient at metabolizing opioids, meaning that the same dosage that was effective in the past may not last as long or may have no effect at reducing pain at all.[18] While further research is needed to fully understand the mechanisms of opioid tolerance, it is possible that some combination of all of these effects is the root cause.
After a person becomes tolerant to opioids, they will need larger doses to feel the same effects they did in the past. Large doses of opioids can cause respiratory depression, a condition where a person’s breathing becomes dangerously slow or stops entirely.[19] If not acted upon quickly, overdosing on opioids can cause death. For this reason, opioids should be taken cautiously and under the supervision of a medical professional. Due to these dangers, opioids are not the first-line treatment for RLS, but they do remain a potential solution when closely monitored.

Treatment for Opioid Use Disorder
If you are struggling with opioid use disorder, you are not alone. Johns Hopkins University has released an interesting point on the opioid epidemic, stating that “About 75% of people in the U.S. who became addicted to street opioids such as heroin during the 2000s report that they started out taking prescription opioid drugs. This trend may be related to availability: In most parts of the United States, fentanyl is cheaper and easier to obtain than prescription opioids.”[2] Unfortunately, there still appears to be much stigma surrounding those who are struggling with opioid use disorder. We are here to encourage you that opioid use disorder is not something that you need to tackle alone, and to seek help for opioid use disorder if you are struggling. Treatments for opioid use disorder exist, and recovery is possible. SAMHSA (the Substance Abuse and Mental Health Services Administration) operates a 24/7, 365-day-a-year treatment helpline for both those who are struggling and their families. They can be contacted at 1-900-662-HELP (4357). Additionally, a number of medications exist to help those who are struggling with OUD, including buprenorphine, methadone, and naltrexone.[20]
For community members who see instances of opioid use disorder in their daily lives, we encourage you to become trained on using Narcan (naloxone), an over-the-counter nasal spray designed to rapidly reverse opioid overdoses. Even just being there and providing support for a person struggling with OUD can make a world of difference.
Conclusion
Although opioids remain an option for treating RLS, they should not be considered as the first course of action. The efficacy of opioids has long been proven, but so have the resulting dangers of addiction and dependence. For those who are currently using opioids to treat their RLS, or who are considering opioids, we urge you to consider other options first. Consult first with your provider if opioids are the right treatment for you, and keep in regular touch with them if you decide to begin using opioids. If you are looking to explore alternative treatments to RLS, the team here at Empower Sleep is ready to help!